SPECIAL FEATURE
February 2025 Volume 24 Issue 1
Fungal infections
Why it matters more than you think
Dr. Aashik Shamas, Dr. Adnan Saood
ShareAmong the five senses, smell remains the most neglected in modern clinical practice. While vision, hearing, touch, and balance are routinely assessed, olfaction is frequently overlooked or dismissed as nonessential. This disregard persists even with growing evidence of the sense of smell’s deep connections to neurological function, systemic health, emotional well-being, and quality of life.
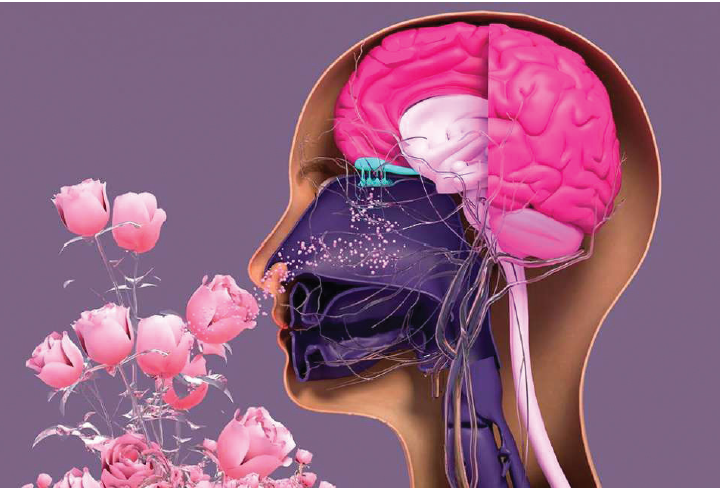
Far from being a minor sensory luxury, olfaction serves as a vital biological system and an important diagnostic tool. Recognizing its clinical relevance is essential for early disease detection, patient safety, and comprehensive medical care.
Despite this, smell is still treated as a secondary sense. Vision and hearing dominate clinical evaluations, and touch, pain, and balance receive structured assessment protocols. But smell rarely receives the same attention. This neglect persists even though olfaction plays a key role in health, disease, and everyday functioning. Smell is a fundamental part of human biology, not merely an optional or a decorative sense. The olfactory pathway connects directly to the limbic system, the brain region responsible for emotion, memory, and behavior. Unlike other sensory modalities, olfactory signals bypass the thalamus and reach deeper brain structures quickly. This explains why certain smells can evoke vivid memories or intense emotional responses. It also explains why loss of smell has consequences that extend well beyond the nasal cavity.
Olfaction also plays a critical role in basic survival. It alerts individuals to smoke, gas leaks, spoiled food, environmental hazards, and many such risks. When smell is impaired, the risk of accidents, foodborne illness, and unnoticed dangers increases significantly. These vulnerabilities often remain unrecognized until harm occurs. In clinical settings, smell is often ignored unless the patient raises a concern. Many do not. Some assume smell loss is a normal part of aging, while others fail to recognize it as an underlying disease. As a result, a valuable diagnostic clue is missed.
Olfactory dysfunction is an early marker of neurological disease. Smell loss may appear years before motor symptoms in Parkinson’s disease. It is also linked to Alzheimer’s disease and other neurodegenerative conditions. In these cases, smell loss reflects early brain involvement rather than nasal pathology. When clinicians ignore this symptom, opportunities for early detection and timely intervention are lost. Smell also reflects systemic health. Chronic inflammation, metabolic disorders, and autoimmune conditions can impair olfactory function. Reduced smell sense is associated with diabetes, chronic kidney disease, and liver disease. Infections can also affect olfactory neurons, sometimes permanently.
The recent attention topost-viral smell loss highlighted how disruptive this symptom can be. The relationship between smell and mental health is equally significant. Smell loss increases the risk of depression and anxiety. Food becomes less appealing, social interactions change, and the enjoyment of daily experiences diminishes. This decline in quality of life is often underestimated. Patients may struggle to describe the change, but the impact is real and persistent. Nutrition is another overlooked area. Smell drives appetite and food choice. When the sense of smell is impaired, patients may eat less, eat poorly, or rely on excess salt and sugar to compensate.
This affects older adults, in particular, increasing the risk of malnutrition and frailty. In hospital settings, smell loss may contribute to poor oral intake, yet it is rarely assessed. Despite its importance, smell testing remains uncommon. Time constraints and limited training play a role. Many clinicians are unfamiliar with simple screening tools. Some still hold the outdated assumption that smell loss has little clinical value. Basic smell assessment is feasible.

Picture: Erin Hendrikx
Simple odor identification tests require only minutes and can be performed in outpatient clinics and wards. They provide objective data and support clinical reasoning. Smell testing does not replace imaging or laboratory work, but it adds valuable context. Treatment options are available. Although some causes of smell loss are irreversible, others respond to intervention. Managing nasal inflammation, adjusting medications, or addressing nutritional deficiencies can improve function. Olfactory training has demonstrated benefit in selected patients. Early identification increases the likelihood of recovery. Smell also deserves attention in public health planning. Environmental pollution can affect olfaction, and occupational exposure to chemicals may damage olfactory receptors. These effects carry longterm consequences. Monitoring smell function could serve as an early indicator of environmental harm. The exclusion of smell from routine care reflects a broader tendency in medicine to prioritize what is easily measured or visibly impaired. Smell is subjective, subtle, and often silent. Yet its absence changes how people live, eat, work, and relate to others. Restoring attention to olfaction does not require major system changes. It requires awareness. Asking about smell should become routine in relevant clinical contexts. Documenting changes over time adds diagnostic value. Teaching trainees to recognize and respect olfactory symptoms builds better diagnostic habits. Smell deserves a place alongside the other senses in modern medical practice. It offers insight into neurological health, systemic disease, nutrition, and mental well-being. Ignoring it narrows the clinical perspective. Including it strengthens patient care. The forgotten sense is not forgotten by patients living with its loss. It should not be forgotten by clinicians either.
[Dr. Aashik Shamas is Assistant Manager, IMT Administration; Dr. Adnan Saood is an IMT Resident, KIMSHEALTH,Trivandrum.]
TAG: